
Automated lamellar keratoplasty (ALK) was a technique to physically remove a refractive lenticule (the lenticule was merely a disc of corneal tissue) from the cornea after lifting a hinged flap and exposing the stroma. A mechanical microkeratome was used to do both steps of the ALK procedure. In the LASIK procedure, the refractive lenticule was ablated with the excimer laser, while the hinged flap was still created with the mechanical microkeratome. In a later iteration, Femto-LASIK involved creation of the hinged flap with a femtosecond laser, and an excimer laser was used to ablate the refractive lenticule. SMILE, a relatively new technique of performing refractive surgery, uses a femtosecond laser for all steps of the keratomileusis procedure. SMILE involves the creation of a refractive lenticule within the cornea using a femtosecond laser, and subsequent extraction of the refractive lenticule from within the cornea. The refractive error that needs to be treated defines the shape of the refractive lenticule to be created. SMILE is therefore a refractive surgery technique which uses only a femtosecond laser to perform the whole refractive surgery procedure. No excimer laser is needed for the whole procedure.
There are two techniques of femtosecond lenticule extraction- FLEx and SMILE1. They differ from each other in the manner in which the lenticule is extracted from within the cornea. FLEx involves the creation and lifting of a hinged flap, along with the cutting of a refractive lenticule. Since FLEx is only an intermediate step in the ultimate journey to SMILE, henceforth, we will only describe the SMILE technique.
FLEx was first described by Sekundo et al2 in 2008. We first described single incision SMILE in 20113, and published the first results. Since 2008, we have treated over 12000 eyes with the SMILE technique in our clinic. Since the laser obtained marketing approval in 2010, over 3 million SMILE procedures have been carried out worldwide.
Currently, SMILE is available to treat myopic errors upto -12.5 Diopters spherical equivalent, with or without astigmatism of up-to -5 Diopters. Clinical trials are underway for the treatment of hyperopia or hyperopic astigmatism of upto +8 D spherical equivalent. Patient selection criteria are similar to LASIK.
The VisuMax femtosecond laser (Fig1) is used for performing the SMILE procedure. The VisuMax is capable of creating refractive lenticules within the cornea with a high degree of accuracy. The VisuMax® software allows the calculation of the refractive lenticule needed to correct for a particular refractive error, and it also automates all stages of the procedure.
Surgical Technique
Patients are treated under aseptic conditions and topical anesthesia, in a manner similar to LASIK. A standard speculum is used to keep the eye open. In the VisuMax Laser System, the laser system remains fixed, while the patient position can be aligned by adjustment of the position of the patient bed with a joystick. The patient’s eye is positioned under a curved contact glass interface during the operation of the femtosecond laser, and it is positioned under a surgical microscope integrated into the system during the phase of surgical manipulation. The eye view is relayed to the surgical microscope eye pieces in both cases to allow for full visual control during the entire procedure.
Once a sterile curved contact glass is attached onto the laser system optical aperture, and the patient positioned some distance below it, the patient is then asked to look at a blinking fixation light, and the patient’s eye is adjusted in relation to the contact glass interface. The surgeon must ensure that the centration is appropriate. After the surgeon is convinced that the centration is within acceptable limits, suction is initiated to hold the cornea against the contact glass interface.There are also well established protocols to adjust for cyclotorsion, in the case of treatment of high astigmatism.
Once the contact interface is fixed, delivery of the femtosecond laser pulses is initiated. Femtosecond laser pulses with typical pulse energy of less than 150 nJ are delivered with a pulse repetition rate of 500 kHz.
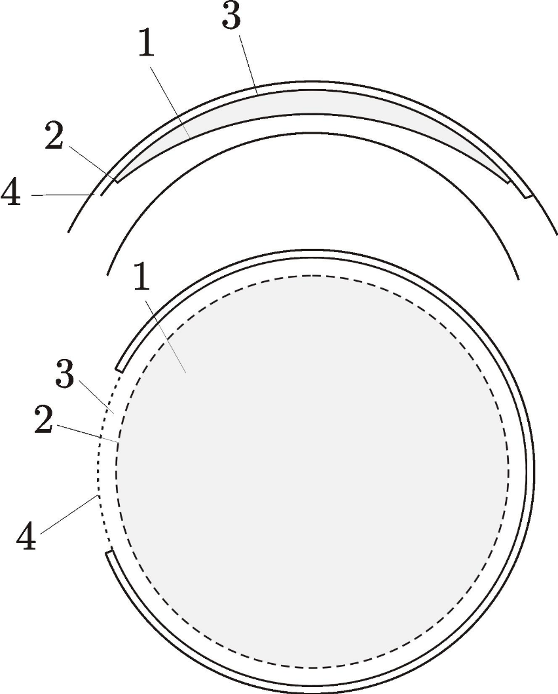
the different tissue disruption planes
Four different tissue disruption planes are created for the SMILE procedure (Fig.2). These four tissue disruption planes include a) the posterior surface of the refractive lenticule, with a pre-programmed diameter based on the optical zone selected b) the 360° cordal length vertical edge of the refractive lenticule, with a depth equivalent to the thickness of the edge of the lenticule c) the anterior surface of the refractive lenticule, which is extended by about 0.5 mm beyond the optical zone desired and finally d) a small 45-110 degree inclination incision of 25-50 degrees in cordal length (2-5mm in arc length) from the surface of the cornea with a depth up to the edge of the anterior part of the lenticule . The entire procedure takes 20-30 seconds, practically independent of the refractive error to be corrected. The sphero-cylindrical shape of the lenticule generated thus is designed to correct for refractive errors. The anterior surface of the lenticule (which is also the undersurface of the cap) can be programmed to be 80 microns or more below the corneal surface, similar to the flap thickness in LASIK. The lenticule diameter can be 5.00 to 7.00 mm, while treating myopia and myopic astigmatism. The minimum thickness of the lenticule edge is 10-15 µm to support easier manual manipulation of the lenticule edge. The side cut incision can be 2-5 mm in arc length, depending on the dexterity and experience of the surgeon.
The parameters mentioned above represent our current clinical experience. All parameters are computer controlled and can be adjusted in the treatment planning step.
Once the femtosecond laser cutting procedure (treatment mode) is finished, the suction is switched off automatically, and the patient’s eye is released from the contact glass and moved under the microscope (observation mode, Fig 3A). The side cut incision is generally created superiorly or superior-temporally, to preserve the nasal and temporal nerve arcades, and to provide surgical convenience.

A small sharp tipped instrument is used to open a small portion of the side cut incision. A small blunt spatula is inserted into the side cut incision, and the anterior surface of the lenticule separated from the overlying cornea (Fig 3B). A small sharp instrument is then used to enter into the tissue disruption plane on the posterior side of the lenticule to separate the edge of the lenticule (Fig 3C). A blunt spatula is then inserted through this edge below the lenticule and used to separate the posterior part of the lenticule from the underlying stroma (Fig 3D). Once the lenticule is free from both surfaces, a micro-forceps (Shah Forceps for Lenticule Extraction, Segal Optics) is inserted to grasp the lenticule and extract it from the corneal stroma (Fig 3E). After 30 seconds, the speculum is removed. Both eyes can be treated at the same time.
Post-operatively patients are prescribed mild steroids and antibiotics for a week and artificial tear supplements for a period of 4-8 weeks after the procedure.
Advantages of SMILE over Femto-LASIK
There are economic, clinical, and work-flow advantages of an only femtosecond laser procedure like SMILE over-performing Femto-LASIK or conventional LASIK or PRK.
The economic advantages of using an all Femto procedure over femto-LASIK are obvious. You require only one laser to perform the entire refractive surgery procedure, instead of two. This means saving on capital costs, maintenance costs, and consumable costs.
The clinical benefits are critical too. An excimer laser ablates the lenticule required to correct the refractive error. In SMILE, the lenticule is carved out within the cornea by a cutting action. This difference between cutting with the femtosecond laser, as opposed to ablation with the excimer laser is significant. Excimer laser ablation rates are dependent on corneal hydration levels, environmental conditions like humidity and temperature, and on the depth in the stroma at which ablation occurs. The scatter in ablation rates is particularly high, when the ablation depth is large, which explains the greater scatter in the results of treatment of larger refractive errors. The femtosecond laser’s cutting action is not dependent on any of the above factors. The scatter in the thickness of the lenticule is minimized, and it is also independent of the refractive error being treated. For all these reasons, several studies have shown that the refractive predictability with the SMILE procedure is higher than with an excimer laser, particularly for higher amounts of refractive errors.
Furthermore, there is the well-known loss of fluence in the periphery of the treatment zone with the excimer laser, which induces spherical aberration. While most modern excimer lasers compensate for this peripheral energy loss, such compensation does increase the overall ablation depth. With the femtosecond laser, such peripheral energy loss is not a factor at all, and no compensation needs to be carried out, and thus the amount of tissue required per diopter of treatment is smaller than that required with an excimer laser which compensates for the peripheral energy loss.
The total amount of energy laid down into the cornea is also much less (orders of magnitude less) than with an excimer laser. Since there is some evidence that the heat generated by fast excimer lasers has an adverse impact on the healing reaction after LASIK, the low amount of energy used by the SMILE procedure is a welcome clinical benefit. Again, several studies have shown that SMILE has more post-operative stability than Femto-LASIK or LASIK.
Several studies have also shown that SMILE preserves the tear function and corneal sensitivity more than Femto-LASIK, which is to be expected considering the smaller incision. There are also bio-mechanical advantages of SMILE over Femto-LASIK.
Finally, the procedure saves working time, as there is no time required for switching from one laser to another.
In conclusion, SMILE is a promising paradigm for refractive surgery. It offers several advantages over conventional corneal refractive surgery, and is quickly becoming the choice of treatment procedure for all high volume refractive surgeons.
References:
- Shah R, Shah S, Vogelsang H. All in One Femtosecond Laser Refractive Surgery. Techniques Ophthal 2010:8(1): 35-42
- Sekundo W, Kunert K, Russmann C, Gille A, Bissmann W, Stobrawa G, Sticker M, Bischoff M, Blum M. First Efficacy and Safety Study of Femtosecond lenticule extraction for the correction of myopia Six Month Results. J Cataract Refract Surg 2008;34:1513-1520
- Shah R, Shah S, Sengupta S. Results of Small Incision Lenticule Extraction- All in One femtosecond laser refractive surgery. J Cataract Refract Surg 2011;37:127-137