
.jpg)
What is diplopia or double vision?
Diplopia or double vision by definition is the simultaneous perception of two images of a single object that may be displaced in any direction. Other terms could be blurred vision, shadowing, or confusion.
Is it uniocular or binocular diplopia?
The first step to evaluate diplopia is to differentiate between uniocular and binocular diplopias as the management varies completely. If the diplopia disappears on covering either eye the diplopia is binocular. If diplopia is persistent or worsens if one of the eyes is occluded then it’s uniocular diplopia of the other eye.
Uniocular diplopia
Any corneal surface problems like tear film abnormalities, uncorrected astigmatism, early stages of cataract, subluxated lens, or early macular issues can cause uniocular diplopia. A simple pinhole test can confirm the same. The management of this is to address the cause.
Binocular diplopia
Binocular diplopia is double vision typically arising as a result of strabismus or ocular misalignment. Here when the fovea of one eye is directed towards the object of regard, the fovea of the other eye is directed elsewhere and the image of the object falls on an extrafoveal area of the retina.
Causes of binocular diplopia
Binocular diplopia can be associated with comitant or incomitant strabismus. Decompensated phorias and accommodation and convergence related problems are the commonest causes of diplopias associated with comitant strabismus. This type of diplopia might be gradual intermittent and may be aggravated by eye-related tasks and associated with asthenopia. Phorias can decompensate due to ocular causes which can disrupt fusion like the onset of cataract etc.
Diplopia due to incomitant strabismus can be caused by myogenic factors or neurogenic factors. Myogenic causes include trauma, ocular myasthenia, myositis and thyroid ophthalmopathy. They are differentiated by their typical features like limited ocular motility, lid involvement, pain and inflammatory signs and sometimes proptosis. Pupils are never involved and they are very asymmetric. Management includes management of the cause and once stable management of diplopia.
Neurological diplopias are caused by weakness of single or multiple ocular motor cranial nerves namely, the oculomotor nerve, trochlear nerve, and abducent nerve. Causes for nerve palsies vary with age. In children, the causes include viral infection, head trauma, intracranial tumors, or infections. In adults, common causes are vasculogenic conditions like diabetes and blood pressure, followed by head injury and intracranial tumours.
Before managing any acquired diplopia the dangerous life-threatening causes have to be ruled out. Such diplopias are called dangerous diplopias and they may present with pain, proptosis, pupil involvement, and other neurological signs.
Examination of diplopia
The examination of patient with diplopia begins as soon as the patient walks into the clinic. Clues such as abnormal head posture (AHP) in the form of a face turn, head tilt or chin up/down position gives an idea of the ocular misalignment. In addition to the eyes, careful attention should be paid to various other signs such as limb weakness or ataxia, facial deviation, abnormal head or eye movements, asymmetrical prominence of the eyes, drooping of the lids or hoarseness of voice as they may suggest underlying neurological illness.
Tests for ocular misalignment and identification of the paretic muscle
The first and foremost objective of the examination is to identify the paretic muscle(s), which is done by performing a series of tests enumerated below.
Abnormal head posture (AHP): Adoption of a head posture is one of the most effective ways to minimize diplopia. The head is usually turned or tilted to the position where the action of the paretic muscle is least required or rarely, patients with longstanding diplopia might adopt the head posture that makes the images most separated in order to suppress one image more easily.
Corneal light reflex test or the Hirscberg test: A measure of the deviation can be obtained by shining a torchlight when the eyes are in the primary position and measuring the displacement of the light reflex from the pupil (figure 1). Each mm of decentration from the pupil equals 7° of ocular deviation. This gives a gross estimation of the deviation.
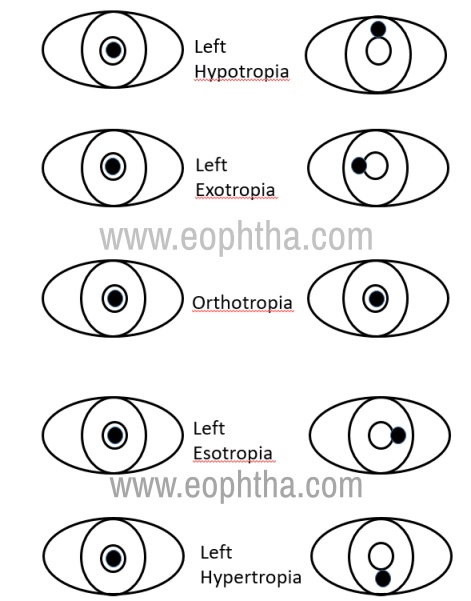
Figure 1: With normal ocular alignment, the light falls in the same position on each cornea relative to the pupil.With a left hypotropia, when the light is placed in the center of the right pupil, the light reflex is above the pupil in the left eye since the right eye is deviated downward relative to the right eye. With an exotropia, when the light is placed in the center of the right pupil, the light reflex is medial to the pupil in the left eye. With an esotropia, when the light is placed in the center of the right pupil, the light reflex is lateral to the pupil in the right eye. With a left hypertropia, when the light is placed in the center of the right pupil, the light reflex is below the pupil in the left eye since the right eye is deviated upwards relative to the right eye.
Cover- uncover test is performed next. It is useful to differentiate the tropias from phorias. The patient is asked to fixate on a target while one eye is occluded. Movement of the uncovered eye to pick up fixation suggests that it is deviated and a tropia is present. If the occluded eye moves when uncovered, it suggests a phoria.
Alternate cover test: Both eyes are alternately covered and then uncovered within seconds while fixating on a target and the movement made by the eye to regain fixation is noted. An esotropic eye moves out to regain fixation and an exotropic eye moves in to fixate. A vertical deviation may be either a hypotropia or a hypertropia, depending on whether the eye moves up or down respectively. It is essential to determine whether the tropia is comitant or incomitant by seeing if the magnitude of the deviation varies with the position of the eye, by which the variation is not seen in the former but present in the latter.
Prism bar cover test is performed to measure the magnitude of the deviation by placing a prism of increasing magnitude over the eyes till movements are neutralized. The primary deviation is the deviation of the misaligned eye when the normal eye is fixating and the secondary deviation occurs when the paretic eye is fixating. A secondary deviation when the paretic eye is fixing is always more the primary deviation. This follows from Hering’s law of equal innervation. The deviation has to be measured in the nine cardinal positions of gaze.
Ductions and versions: Ocular motility has to be tested carefully, individually (ductions), and both eyes together (versions) in all nine cardinal positions. The range of eye movements is examined by asking the patient to follow a target, placed 50 cm away in order to avoid convergence, and the patient should be asked to report any diplopia during the examination. The movements are recorded in an H fashion starting from the primary position, up, down, right, left, up and right, down and right, up and left, and down and left.. This method helps identify the paretic muscle more clearly as each direction corresponds with the main action of a particular extraocular muscle.
Parks three-step test: This test is commonly used to identify the paretic muscle in cases of vertical diplopia. The various steps are:
- To determine which eye is hypertropic in the primary position.
- Then to see whether this hypertropia increases on left or the right horizontal gaze.
- Lastly, to determine whether the hypertropia is worse on head tilting to left or right (Bielschowsky test).
Maddox rod test: is a subjective test of ocular misalignment that requires a cooperative patient and is best suited for small ocular deviations. The Maddox rod, made up of a series of red half-cylinders, is always placed over one eye, say the right eye. The examiner shines a light in front of the patient, and the patient should see a red line perpendicular to the alignment of the Maddox rod with the right eye and the white light with the left eye. A horizontal red line (cylinders aligned vertically) is used to test for vertical ocular misalignment, and a vertical red line (cylinders aligned horizontally) is used to test for horizontal ocular misalignment. If normal alignment of the eyes is present, the red line will pass directly through the white light. If an ocular misalignment is present, the red line will be displaced to the right or left of the white light for a horizontal misalignment or superior or inferior to the white light for a vertical misalignment (Figure 2). Once the direction of the misalignment in primary position is established, the size of the misalignment in each pertinent direction of gaze should be assessed to determine comitance or incomitance.
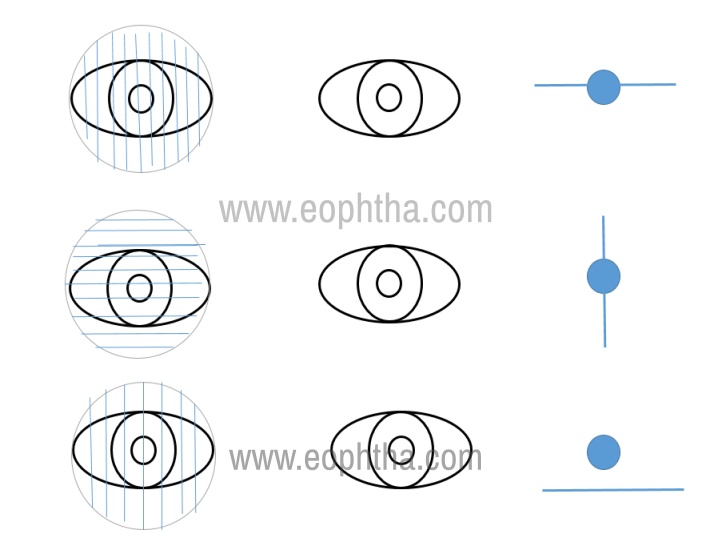
Figure 2: When the Maddox rod is placed vertically over the right eye, the patient should see a horizontal red line and a white light. When the Maddox rod is placed horizontally over the right eye, the patient should see a vertical red line and a white light. If the eyes are aligned, the red line will go through the white light. If the eyes are not aligned, the red light will be deviated in the opposite direction of the eye relative to the white light. For example, with a right hypertropia, the patient will see the red line deviated below the white light.
Double Maddox rod test: This is used to test for torsional misalignments. Maddox rod filters are placed in front of both the eye in a trial frame. The patient sees oblique lines in the presence of torsional diplopia. The cylinders are rotated till the patient fuses and see a single image. The reading in degrees gives an estimate of the amount of torsional misalignment.
Diplopia charting: This test is performed by placing a plain red filter in front of the right eye and a green filter in front of the left eye to dissociate the eyes. The patient is made to sit straight in a semi-dark room and a linear light is then projected from a distance of 4 feet in front of the patient. The light is then moved into all the 9 cardinal positions of gaze. At each position, the patient is asked whether he sees the two lines as fused or separate. If separately, then the distance of separation between the two lines is asked and whether there is horizontal or vertical or torsional separation between the two lines. In cases of perfectly aligned eyes, the patient will be able to fuse the two lines. The position in which the double vision appears and the distance of separation between the two lines is maximum should be noted. This indicates the field of the gaze of the paretic muscle and the distant image belongs to the paretic eye.
The direction of the image is always opposite to the direction of the deviating eye. Therefore, esotropia produces an uncrossed diplopia, exotropia produces a crossed diplopia. Similarly, the hypertropic eye will see the image lower and hypotropic eye will see the image higher; same pattern for the torsions also (figure 3).
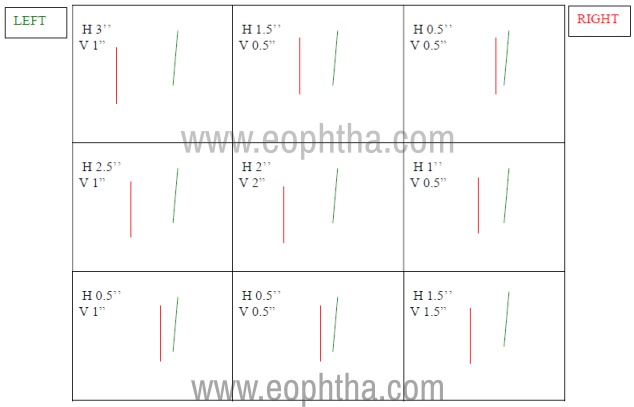
Figure 3: Depicting a diplopia charting done with red in front of right eye and green in front of the left eye showing crossed diplopia. A vertical and torsional component is also seen in all gazes.
Quantitative measurement of the action of extra-ocular muscles
Hess screen test: is a haploscopic test based on the Burian principle that is commonly used to provide a pictorial and reproducible record of the patients’ eye movements. The patient is seated facing the screen being plotted, with the head centred on the fixation spot. Each eye is plotted in turn for the central fixation spot by targets at 15˚and 30˚eccentricity, respectively. Both the eyes are dissociated by the means of red and green glasses and the green glasses is placed in front of the testing eye. The eye behind the red glass is the fixing eye and the eye behind the green glass is the indicating eye. The chart plotting is based on the Hering’s law of equal innervation and Sherrington law of reciprocal innervation. Some general rules for interpreting a Hess chart are as follows:
- The smaller field belongs to the paretic eye
- Neurogenic pareses will show the largest underaction in the direction of paretic muscle and the largest over-action is seen in the contralateral synergist
- Mechanical defects show a compressed field without obvious over-action.
This test can be used for diagnosis as well as follow up of the patient to look for signs of recovery. Figure 4 shows a Hess chart for a lateral rectus palsy.
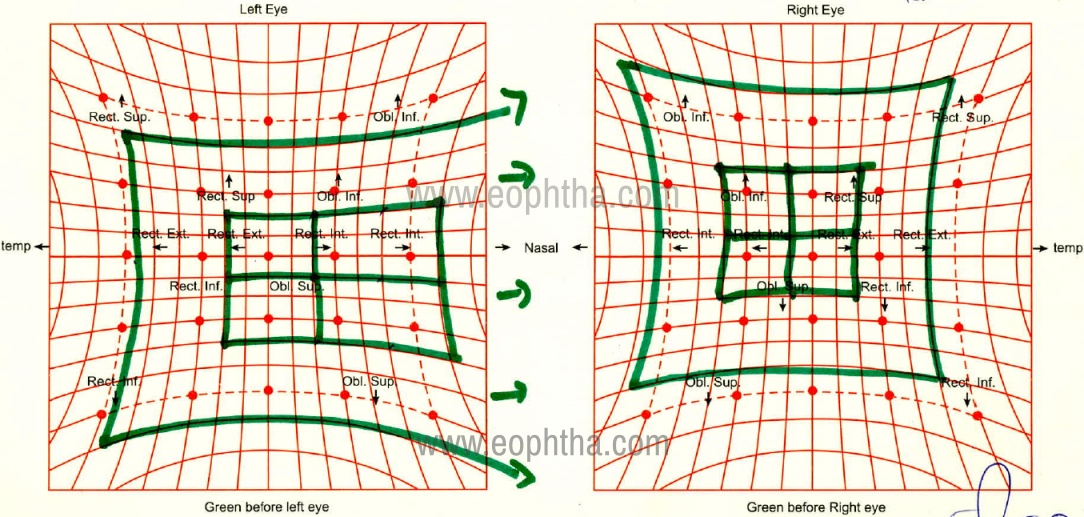
Figure 4: Depicting a right lateral rectus palsy. The inner red dots correspond to the central 15-degree field and outer ones correspond to the 30-degree field. When the green glass is before the left eye, the field for the right eye is being plotted. The right eye here shows gross underaction of the lateral rectus muscle (involved muscle) and unopposed overaction of the medial rectus muscle (contralateral synergist).
Lancaster red-green test: is also based on the haploscopic principle. It is performed in front of a red-green screen that contains horizontal and vertical lines forming squares of 7 cm. The patient is seated at 1 meter from the chart wearing read green glasses and is asked to fixate on the central square and given a green flashlight that casts a linear image. The examiner has a similar red flashlight which he shines on the central square by standing behind the patient and asks the patient to superimpose the his greenlight over the red one. This is then repeated in all the positions of the gaze. The distance between the two streaks of light represents the measurement of the deviation and the results are plotted on a screen. It is interpreted similar to the diplopia charting.
Lees screen test: This test is a modification of the original Hess chart and consists of two tangentially placed screens placed at a right angle to each other with a plane mirror bisecting the right eye. The interpretation is similar to that of a Hess screen chart.
Forced duction test (FDT) and force generation test (FGT) :
Forced duction is to test resistance to passive movement of the eye when active movement is limited. If it’s positive it implies a restrictive pathology as seen in thyroid ophthalmopathy, muscle entrapment following trauma, and long-standing nerve palsies. If it’s negative it suggests a paralysis of the nerve controlling the muscle action. This differentiation is crucial to diagnosis as well as surgical planning.
Force Generation test (FGT) is performed to assess if there’s residual muscle function in a paretic muscle. A forceps is placed and the eye held by grasping the conjunctiva. The patient is asked to look towards the direction of action of the paretic muscle. The presence and strength of the tug felt on the forceps gives information about the presence of residual muscle action.
Management of diplopia:
Temporary management:
- Uniocular occlusion – used in acute neurogenic diplopias while waiting for investigations and then stability. This can be done by using frosted glasses or Bangarter’s foils
- Prisms – after the acute phase when angles are small prisms are a comfortable option. They can be used as ground-in prisms in glasses if angles are up to 6 prisms in each eye. Larger angles require stick-on prisms called Fresnel prisms for angles up to a maximum of even 40 prisms.
Definitive management:
Surgical management – once angles are stable as confirmed by stable measurements and Hess charts if patients have a good ability to fuse with prisms surgical options are considered. Adjustable suture techniques offer better outcomes in most of these situations. Residual small deviations after surgeries do well with small prisms.
Intractable diplopias:
There’s a small but definite subset of patients who have diplopias that are intractable. Such patients have no ability to fuse despite motor alignment. The common causes for this can be central disruption of fusion which is typically seen in patients with long-standing uncorrected unilateral vision problems like unilateral aphakias. Other causes are diplopias due to macular pathologies causing image distortion following retinal surgeries or aniseikonia. It is very important to look for intractable diplopias using prisms before considering surgery for ocular deviations. In situations where patients demand surgery for improvement of deviations occlusion contact lenses can help with managing the diplopia.
References
- Kanski, J. J., Bowling, B., Nischal, K. K., & Pearson, A. (2011). Strabismus. Chapter 18.Clinical ophthalmology: A systematic approach(7th ed.). Edinburgh ; New York: Elsevier/Saunders.
- Rucker JC, Tomsak RL. Binocular diplopia: A practical approach. The Neurologist. 2005;11(2):98-110.
- Danchaivijitr C, Kennard C. Diplopia and eye movement disorders: A practical approach. J Neurol Neurosurg Psychiatry 2004;75(Suppl IV):24–31.
- Sreedhar A, Menon A. Understanding and evaluating diplopia. Kerala J Ophthalmol 2019;31:102-11.
- Friedman DI. Pearls: Diplopia. Semin Neurol. 2010;30(1):54-65.